Keratosis refers to the presence of keratin on an epithelial surface, normal in some areas such as skin, and abnormal in others such as the larynx (a.k.a. the voice box). Many keratoses, such as in the larynx, are flat and may be described by the clinician as a vocal cord nodule or leukoplakia. Microscopically, there may be difficulty in distinguishing verrucal keratosis from verrucous carcinoma, especially in a small biopsy of the larynx.
Microscopically, verrucal keratosis shows a heavily keratinized surface. The presence of abundant keratohyalin granules in the stratum granulosum is characteristic and helps differentiate the lesion from verrucous carcinoma which characteristically demonstrates no granules, or few. Rete pegs in verrucal keratosis tend to be elongated, relatively thin and pointed in contrast to those of verrucous carcinoma which are elongated, bulbous and thick and appear to be “pushing.” Dysplasia may be present in verrucal keratosis but is lacking in verrucous carcinoma. Submucosal chronic inflammation is more marked in verrucous carcinoma than in verrucal keratosis. Koilocytosis (see “Wart” for illustration) is common in verrucal keratosis but usually absent in verrucous carcinoma.
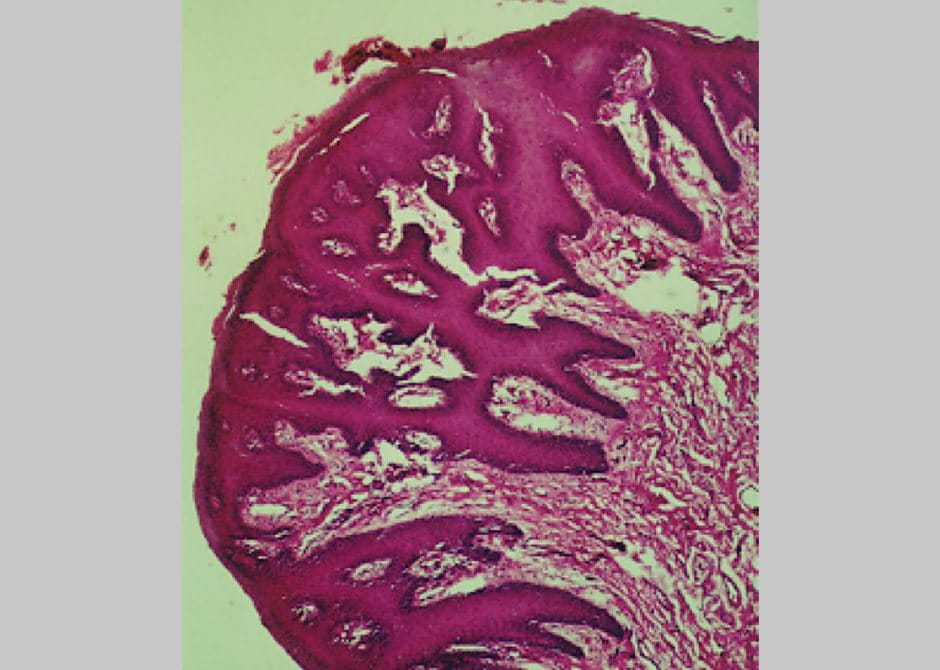
Examples of verrucal keratosis
Verrucal keratosis on the forehead
Note the heavily keratinized surface with papillary projections reminiscent of the “church spires” (double arrows) also described with verrucous carcinoma. Rete pegs are elongated, thin and pointed (single arrows).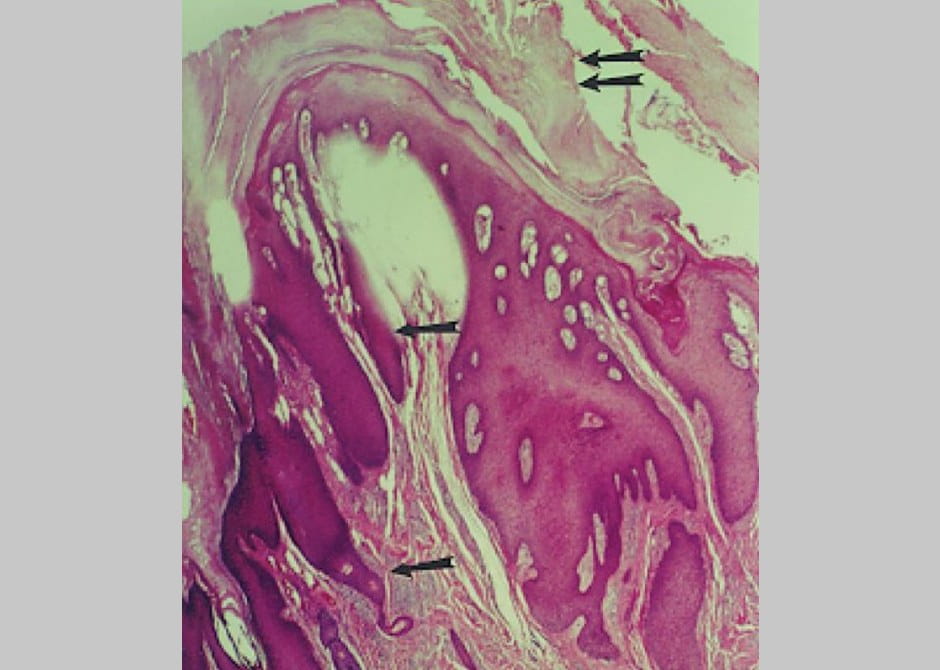
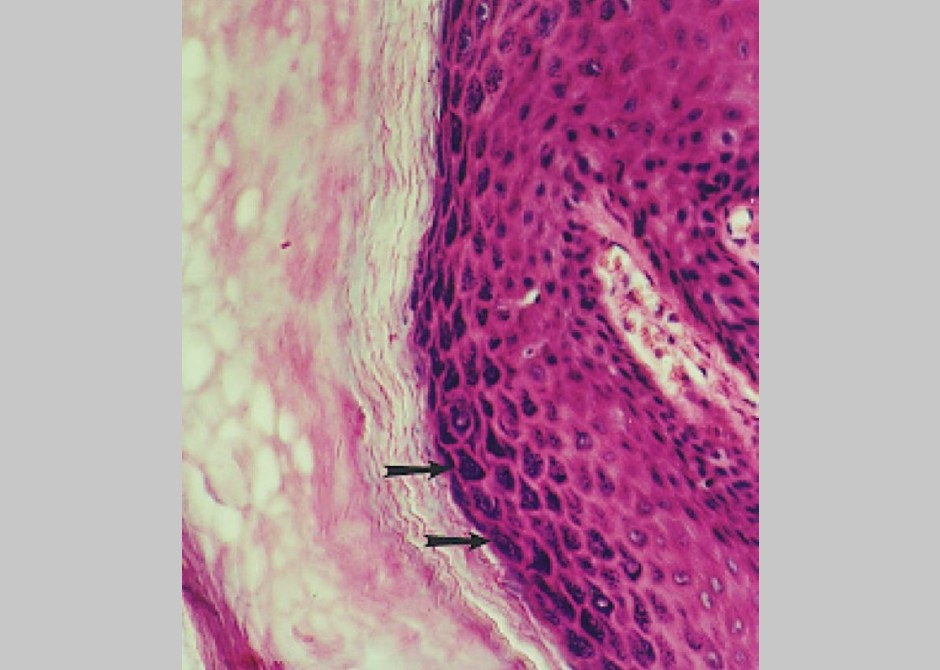
Verrucal keratosis on the forehead
Extremely prominent collection of keratohyalin granules (arrows) in the granulosal cell layer that is generally absent in verrucal carcinoma. Keratin has formed abundantly on the surface.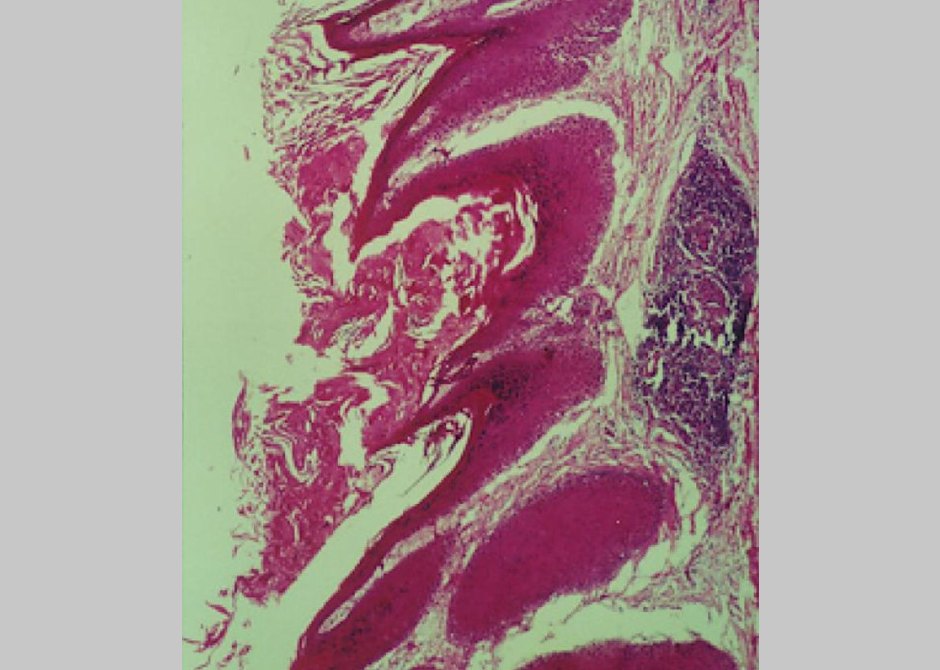
Verrucal keratosis on the gingiva
Church-spire like formation of keratin, relatively narrow rete pegs, and one isolated focus of inflammatory cells.